What are you looking for?
Search





 Source: PubChem Source: PubChem |
Sequence: AXAWFK Molecular Formula: C45H55N9O6 Molecular Weight: 817.98 g/mol CAS Number:158861-67-7 PubChem CID’╝Ü6918245 Synonyms: Pralmorelin’╝øpralmorelina’╝øKP-102’╝øpralmoreline |
Ō¢ÄGHRP-2 Research
What is the research background of GHRP-2? Growth hormone plays a pivotal role in human growth, development, and metabolic balance. Scientists have long sought substances capable of effectively regulating its secretion. Growth hormone-releasing peptides (GHRPs), a class of synthetic oligopeptides that stimulate growth hormone release, have emerged as a focus of research. GHRP-2 mimics the action of ghrelin by binding to the ghrelin receptor, activating signaling pathways to efficiently stimulate GH release. It demonstrates potential in diagnosing and treating growth hormone deficiency, intervening in anorexia, and protecting against organ damage, driving deeper research into its mechanisms and applications. What is the mechanism of action for GHRP-2? Regulation of Growth Hormone Secretion Acting on the Hypothalamic-Pituitary Axis: GHRP-2 stimulates growth hormone (GH) release through a unique dual-complementary action targeting both the hypothalamus and pituitary gland (Bowers C Y). At the pituitary level, GHRP-2 binds to the growth hormone-releasing hormone receptor (GHS-R). Upon binding to GHS-R, GHRP-2 initiates a cascade of intracellular signaling events. For instance, it activates phospholipase C (PLC), which catalyzes the hydrolysis of phosphatidylinositol-4,5-bisphosphate (PIP2) on the cell membrane into inositol trisphosphate (IP3) and diacylglycerol (DAG). IP3 promotes calcium ion release from the endoplasmic reticulum, while DAG activates protein kinase C (PKC), ultimately leading to GH release (Roh S G,). In a study using bovine pituitary cells, GHRP-2 at various concentrations (10Ōü╗ŌŖā1;ŌŖā3; to 10Ōü╗ŌüĘ M) significantly increased GH secretion (P < 0.05), indicating a direct stimulatory effect of GHRP-2 on GH secretion by pituitary cells [1]. Synergistic Action with Growth Hormone-Releasing Hormone (GHRH): GHRP-2 exhibits synergistic effects with GHRH in stimulating GH release. When co-administered to pituitary cells, they act through distinct signaling pathways that ultimately converge to promote GH secretion. Studies indicate that GHRH primarily activates adenylate cyclase (AC), elevating intracellular cAMP levels to subsequently activate protein kinase A (PKA), thereby promoting GH gene transcription and GH synthesis/release. Conversely, GHRP-2 exerts its effects via the PLC-IP3/DAG-PKC pathway described above. Their synergistic interaction significantly increases GH release. In sheep pituitary cell experiments, both GHRH (10 nM) and GHRP-2 (100 nM) individually increased GH mRNA levels and GH release in a time-dependent manner within 0.5ŌĆō2 hours; this effect was markedly enhanced when combined [2]. Regulation of Growth Hormone Secretion: GHRP-2 stimulates growth hormone (GH) release through a unique dual-complementary action, simultaneously targeting the hypothalamus and pituitary gland (Bowers CY). At the pituitary level, GHRP-2 binds to the growth hormone-releasing hormone receptor (GHS-R). Upon binding to GHS-R, GHRP-2 initiates a cascade of intracellular signaling events. For instance, it activates phospholipase C (PLC), which catalyzes the hydrolysis of phosphatidylinositol 4,5-bisphosphate (PIP2) on the cell membrane into inositol trisphosphate (IP3) and diacylglycerol (DAG). IP3 promotes calcium ion release from the endoplasmic reticulum, while DAG activates protein kinase C (PKC), ultimately leading to GH release (Roh S G,). In a study using bovine pituitary cells, GHRP-2 at various concentrations (10Ōü╗ŌŖā1;ŌŖā3; to 10Ōü╗ŌüĘ M) significantly increased GH secretion (P < 0.05), indicating a direct stimulatory effect of GHRP-2 on GH secretion by pituitary cells [1]. Therapeutic Effects on Anorexia: For patients with anorexia, intranasal administration of GHRP-2 increases hunger sensation and food intake, reduces early satiety, and improves hypoglycemia symptoms. After 14 months of GHRP-2 administration, patients gradually gained 6.7 kg in body weight. The mechanism may involve GHRP-2 acting as a ghrelin receptor agonist to mimic ghrelin's effects, thereby modulating the appetite center and improving patients' eating behavior and nutritional status [3].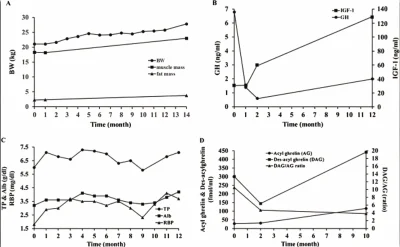 Figure 1 (A) Changes in body weight, muscle mass, and fat mass after treatment with growth hormone releasing peptide-2 (GHRP-2). Fat and muscle mass were evaluated using the bio-impedance method. All parameters gradually increased, with body weight and daily energy intake rising by ŌłÆ1.5 to 2.4 kg and 12% to 36%, respectively, after ghrelin infusion. (B) Changes in growth hormone (GH) and insulin-like growth factor 1 (IGF-1) levels following GHRP-2 treatment. GH decreased while IGF-1 increased after 12 months. (C) Changes in nutritional status. Retinol binding protein (RBP) and total protein (TP) rose rapidly, with albumin (Alb) increasing after 4 months. These parameters further increased after 12 months. (D) Changes in acyl ghrelin (AG) and des-acyl ghrelin (DAG) levels after GHRP-2 administration. Fasting DAG and AG increased, and the DAG/AG ratio decreased after 10 months. BW; body weight. Source: PubMed
[3]
What are the medical applications of GHRP-2? Diagnosis of growth hormone secretion deficiency: GHRP-2 is clinically used as a diagnostic agent for growth hormone deficiency. For adult growth hormone deficiency, the international first-line diagnostic test is the insulin tolerance test (ITT). However, due to its potential to cause serious adverse events, it is contraindicated for some patients. Studies have proposed using GHRP-2 to diagnose adult growth hormone deficiency (GHD). The study enrolled 77 healthy subjects and 58 patients with peak GH < 3 ╬╝g/L as determined by ITT. All subjects received an intravenous injection of 100 ╬╝g GHRP-2, followed by blood sampling over the subsequent 2 hours. GH levels were measured using an immunoradiometric assay. Results showed that all subjects exhibited peak serum GH within 60 minutes post-GHRP-2 administration. GH responsiveness to GHRP-2 was unaffected by gender. Although responses were slightly lower in elderly subjects and obese individuals, this did not compromise GHD diagnosis. Repeat testing demonstrated good reproducibility of this method. When using GHRP-2 to diagnose GHD, a cutoff value of 15 ╬╝g/L corresponds to the diagnostic value of 3 ╬╝g/L in the ITT, indicating that setting an appropriate serum GH concentration cutoff reliably diagnoses severe growth hormone deficiency
[4]. Treatment of Anorexia: For patients with a long history of anorexia, GHRP-2 may represent a promising therapeutic agent. One study administered GHRP-2 intranasally before each meal for one year to a patient with a 20-year history of anorexia. Prior to treatment, although the patient's fear of eating and desire to be thin had diminished through previous therapies, gastrointestinal dysfunction prevented increased food intake and weight gain. Symptoms included postprandial vomiting, constipation, sub-intestinal obstruction, and hypoglycemia. Following GHRP-2 administration, the patient experienced increased hunger and food intake, reduced early satiety, hypoglycemia symptoms improved, and body weight gradually increased by 6.7 kg (from 21.1 kg to 27.8 kg) within 14 months of initiating treatment. Fatigue and muscle strength improved, physical and mental activity increased, and no significant side effects were observed with long-term intranasal administration. This suggests GHRP-2 may be an effective therapeutic agent for patients with severe chronic anorexia
[3]. Alleviating Burn-Induced Dysfunction: Following severe burns, increased production of catabolic hormones and inflammatory cytokines alongside decreased anabolic hormone levels leads to metabolic hyperactivity, reduced lean body mass, and muscle wasting. Although various therapies such as exercise and the use of anabolic hormones (insulin, growth hormone, IGF-I, or steroids) have been proposed or employed, their effects remain suboptimal. Experimental results indicate that the newly isolated anti-cachexia peptide ghrelin is downregulated in post-burn rats. Exogenous ghrelin can restore weight loss by increasing food intake and enhancing muscle mass in mice. It also significantly reduces skeletal muscle protein degradation in burn rats by normalizing muscle mRNA expression of E3 ubiquitin ligase, MuRF1, and MAFbx. The short half-life of ghrelin limits its clinical application. In contrast, the synthetic hexapeptide growth hormone-releasing peptide 2 (GHRP-2) is a stable and potent GHRP receptor agonist that increases body weight in rodents, exhibits anti-inflammatory effects in arthritic rats, and improves catabolic metabolism in critically ill patients. GHRP-2 positively influences body weight, food intake, and skeletal muscle protein breakdown in burned rodents, mitigating burn-induced dysfunction [5].
Conclusion GHRP-2 activates growth hormone secretion by stimulating relevant signaling pathways through its action on GHS-R within the hypothalamic-pituitary axis. Medically, it can diagnose growth hormone deficiency and treat conditions such as anorexia, septic acute kidney injury, and post-burn dysfunction, while also exhibiting analgesic and antioxidant effects.
About The Author The above-mentioned materials are all researched, edited and compiled by Cocer Peptides.
Scientific Journal Author Haruta I is a clinician-scientist affiliated with the Department of Psychosomatic Internal Medicine at Kagoshima UniversityŌĆÖs Graduate School of Medical and Dental Sciences in Japan. Her translational research focuses on endocrine and metabolic interventions in severe anorexia nervosa. Haruta I is listed in the reference of citation [3].
Figure 1 (A) Changes in body weight, muscle mass, and fat mass after treatment with growth hormone releasing peptide-2 (GHRP-2). Fat and muscle mass were evaluated using the bio-impedance method. All parameters gradually increased, with body weight and daily energy intake rising by ŌłÆ1.5 to 2.4 kg and 12% to 36%, respectively, after ghrelin infusion. (B) Changes in growth hormone (GH) and insulin-like growth factor 1 (IGF-1) levels following GHRP-2 treatment. GH decreased while IGF-1 increased after 12 months. (C) Changes in nutritional status. Retinol binding protein (RBP) and total protein (TP) rose rapidly, with albumin (Alb) increasing after 4 months. These parameters further increased after 12 months. (D) Changes in acyl ghrelin (AG) and des-acyl ghrelin (DAG) levels after GHRP-2 administration. Fasting DAG and AG increased, and the DAG/AG ratio decreased after 10 months. BW; body weight. Source: PubMed
[3]
What are the medical applications of GHRP-2? Diagnosis of growth hormone secretion deficiency: GHRP-2 is clinically used as a diagnostic agent for growth hormone deficiency. For adult growth hormone deficiency, the international first-line diagnostic test is the insulin tolerance test (ITT). However, due to its potential to cause serious adverse events, it is contraindicated for some patients. Studies have proposed using GHRP-2 to diagnose adult growth hormone deficiency (GHD). The study enrolled 77 healthy subjects and 58 patients with peak GH < 3 ╬╝g/L as determined by ITT. All subjects received an intravenous injection of 100 ╬╝g GHRP-2, followed by blood sampling over the subsequent 2 hours. GH levels were measured using an immunoradiometric assay. Results showed that all subjects exhibited peak serum GH within 60 minutes post-GHRP-2 administration. GH responsiveness to GHRP-2 was unaffected by gender. Although responses were slightly lower in elderly subjects and obese individuals, this did not compromise GHD diagnosis. Repeat testing demonstrated good reproducibility of this method. When using GHRP-2 to diagnose GHD, a cutoff value of 15 ╬╝g/L corresponds to the diagnostic value of 3 ╬╝g/L in the ITT, indicating that setting an appropriate serum GH concentration cutoff reliably diagnoses severe growth hormone deficiency
[4]. Treatment of Anorexia: For patients with a long history of anorexia, GHRP-2 may represent a promising therapeutic agent. One study administered GHRP-2 intranasally before each meal for one year to a patient with a 20-year history of anorexia. Prior to treatment, although the patient's fear of eating and desire to be thin had diminished through previous therapies, gastrointestinal dysfunction prevented increased food intake and weight gain. Symptoms included postprandial vomiting, constipation, sub-intestinal obstruction, and hypoglycemia. Following GHRP-2 administration, the patient experienced increased hunger and food intake, reduced early satiety, hypoglycemia symptoms improved, and body weight gradually increased by 6.7 kg (from 21.1 kg to 27.8 kg) within 14 months of initiating treatment. Fatigue and muscle strength improved, physical and mental activity increased, and no significant side effects were observed with long-term intranasal administration. This suggests GHRP-2 may be an effective therapeutic agent for patients with severe chronic anorexia
[3]. Alleviating Burn-Induced Dysfunction: Following severe burns, increased production of catabolic hormones and inflammatory cytokines alongside decreased anabolic hormone levels leads to metabolic hyperactivity, reduced lean body mass, and muscle wasting. Although various therapies such as exercise and the use of anabolic hormones (insulin, growth hormone, IGF-I, or steroids) have been proposed or employed, their effects remain suboptimal. Experimental results indicate that the newly isolated anti-cachexia peptide ghrelin is downregulated in post-burn rats. Exogenous ghrelin can restore weight loss by increasing food intake and enhancing muscle mass in mice. It also significantly reduces skeletal muscle protein degradation in burn rats by normalizing muscle mRNA expression of E3 ubiquitin ligase, MuRF1, and MAFbx. The short half-life of ghrelin limits its clinical application. In contrast, the synthetic hexapeptide growth hormone-releasing peptide 2 (GHRP-2) is a stable and potent GHRP receptor agonist that increases body weight in rodents, exhibits anti-inflammatory effects in arthritic rats, and improves catabolic metabolism in critically ill patients. GHRP-2 positively influences body weight, food intake, and skeletal muscle protein breakdown in burned rodents, mitigating burn-induced dysfunction [5].
Conclusion GHRP-2 activates growth hormone secretion by stimulating relevant signaling pathways through its action on GHS-R within the hypothalamic-pituitary axis. Medically, it can diagnose growth hormone deficiency and treat conditions such as anorexia, septic acute kidney injury, and post-burn dysfunction, while also exhibiting analgesic and antioxidant effects.
About The Author The above-mentioned materials are all researched, edited and compiled by Cocer Peptides.
Scientific Journal Author Haruta I is a clinician-scientist affiliated with the Department of Psychosomatic Internal Medicine at Kagoshima UniversityŌĆÖs Graduate School of Medical and Dental Sciences in Japan. Her translational research focuses on endocrine and metabolic interventions in severe anorexia nervosa. Haruta I is listed in the reference of citation [3].
Richard A. Loy US
I wish I had found this when I started. Things I learned the hard way and that you shouldn't do with Retatrutide: 1- Not drinking enough fluids and not including mineral salts and electrolytes. You dehydrate very quickly with Retatrutide. 2- Cutting calories by more than 1000 kcal was crazy, and I lost almost as much muscle as fat. Remember that Retatrutide increases your basal metabolic rate. 3- Not getting enough protein (I always did this correctly, but many people make mistakes). Aim for 2 grams per kilogram of body weight of muscle mass. 4- Starting with very high doses or increasing them too quickly. I was cautious and started with 0.5 mg and then spent 4 weeks on 1 mg. 5- Thinking it's Tirze or Sema; it's not the same at all. Appetite suppression is less pronounced, and Retatrutide works in the long term. 6- Not weight training; this is a very common mistake. I love it, but a lot of people make mistakes here. I think that training, along with protein, is vital for maintaining mu
04.22.2026 5
 Retatrutid 1kits(10Vials)
Retatrutid 1kits(10Vials)

Larry K. Goheen US
32M - Athletic/sports background - I have done about 2-3 days per week lifting/cardio: 30min-1hr. Not strict with it. I went from 2-4-6-8 each month and I've stayed at 8mg. Mots at 2mg 3x weekly. My diet consists of mostly protein and complex carbs. both healthy and unhealthy sources. I don't count calories. Tbh for being as inconsistent as I've been with diet and training, I'm surprised and content with these results. Reta is a most excellent tool!
04.09.2026 7
Retatrutid 1kits(10Vials)
Albert US
I have been on Retatrutide since January. I have been on Semaglutide and Trizepitide in the past under brand names. I have found Reta, and it’s worked the best for me. I have lost 37 pounds using Reta without the monthly increases that are within the studies. It doesn’t make me feel miserable. I have experience very very minimal side effects. And honesty I can’t see myself ever changing.
04.09.2026 7
Retatrutid 1kits(10Vials)
Martin Lucas US
Hey all. I started retatrutide through a friend about 4 months ago and the success has been astounding. I've lost 60 lbs so far (267-208 as of today) and feel much better about myself and the progress I've made in multiple facets of life. I found this place and have been lurkin for a while just taking information in and figured I'd finally post something. Thank you all for the valuable insight and for more to come.
04.06.2026 6
Retatrutid 1kits(10Vials)

Vivian C. Walsh US
I have been taking retatrutide for a few weeks and I had the effects (atleast the weight loss mainly) (hard to say if it was mainly from the hard work put in though) I have already purchased the goods from SH., I was using 13mm needles and now I have some 12.7mm ones (the ones supplied from UK pharmacies) I was wondering if these are too large/long - I know a lot of people use 8mm, could I just choose not to insert the whole needle? Or what angle would be best, I do have a decent amount of belly fat so I believe angled the 12.7mm should work - just wondering if any advice ! Thanks
02.25.2026 5
Retatrutid 1kits(10Vials)
Carlos US
This was my 6th order with SH, arrived in 8 days to the UK, as standard for them. I am delighted.
02.12.2026 4
Retatrutid 1kits(10Vials)

You have successfully commented, please wait for review
Copied Successfully
You can enjoy up to 1 free gift!

Customer Reviews
Real feedback from buyers all over the world, real experience, trustworthy!